A roadmap for community transformation
by ariel_domlyn August 11, 2021Nobody ever said change is easy. Community-level change is our best bet for chipping away at pervasive health inequities, yet each community is nestled inside local, regional and national attitudes, policies, and expectations. Can such diverse systems be changed? Yes, but it requires not just change – but a total transformation.
Editor’s note: This piece was originally published by the Institute for Healthcare Improvement here on August 3, 2021, and has been reposted here with the authors’ permission
One initiative from IHI (in partnership with Communities Joined in Action, Community Solutions, and Network for Regional Healthcare Improvement) faced this challenge of assisting community transformation by developing a roadmap for achieving a culture of health. The development, use, and evaluation of this roadmap is described in a new publication in the American Journal of Orthopsychiatry by a handful of partners involved in its development: portions of this post are drawn from this publication, the full text of which can be found here.
The Spreading Community Accelerators through Learning and Evaluation (SCALE) initiative helped communities around the United States shift away from focusing on the problems to embrace adaptation, abundance, and connection to become a Community of Solutions. Based in the literature of sustainable development, being a Community of Solutions requires three behaviors as critical conduits of change: Relationships, Improvement, and Equity. Relationships are defined as how people relate to themselves, each other, and to those affected by inequity. Improvement refers to how the community approaches the change process. Equity describes how the community creates abundance through leadership, adaptability, empowerment, and connection. Collectively, becoming a Community of Solutions intends to transform communities into places where health is a shared value, there are thriving cross-sector partnerships, and there is improvement in population health, wellbeing, and equity.
The Community Transformation Map
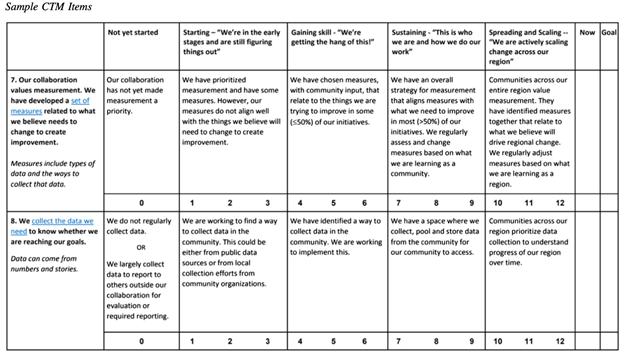
The complexities of community relationships, improvement, and equity are distilled into a 40-item tool for assessing and planning community transformation: The Community Transformation Map (CTM). It took nearly a year for the CTM to be developed and refined by a SCALE workgroup of implementation scientists, evaluation experts, and community leaders. The workgroup scanned the community change literature for similar tools, cross-referenced items against these resources, and conducted multiple feedback rounds with participating community coalitions.
Each item is graded on five levels depending on whether the community has not yet started to transform this aspect of their community, are in the early stages of change, are gaining skills, have sustained this aspect of transformation, or are spreading and scaling up this aspect to other regions or communities. Sample items are below.
How is the CTM used?
The CTM brings community members together to reflect, reconcile perspectives, and chart an action plan. As the authors of the recent American Journal of Orthopsychiatry article state:
“The CTM is intended to foster a holistic view of community coalition functioning from the perspective of system leaders, community facilitators, and community residents with lived experiences of inequities. Therefore, respondents should include community members across hierarchical structures and leaders with lived experience of inequities. During assessment, each member of the coalition first considers each CTM item from a personal perspective and assigns a score (from 1 to 12) for both the current capability level (‘Now’) and for where the member would like to see the community be in six months (‘Goal’). Individual ratings are then compared by participants in a collaborative discussion session and discrepancies of score differences (of five or more points) are reconciled. In translating the CTM from assessment to action, individual items are reflected upon by visually inspecting high/low scores and gaps a between ‘Now’ and ‘Goal’ scores. Priorities are determined by the coalition members.”
Each coalition self-administers the CTM semiannually and uses the information to revise their improvement plans.
Is the CTM helpful to communities?
The first cohort of community coalitions that used the CTM completed it twice a year for two years. Interviews showed a favorable perception of the CTM, stating for example: “[It] actually gave a structure to the discipline we needed to keep going and saying: ‘Are we where we want to be? Are we doing what we want to be doing? Are we making a difference?’” The greatest value is in breaking down the complexities of transformative change into digestible, actionable pieces.
The article offers an example of how the CTM was used by one coalition:
“After the first administration [Coalition 3] selected ‘shared stewardship’ (a Relationship construct) as a priority area. This included three items: ‘There is a shared commitment to health, well-being, and equity across the community (baseline ‘Now’ rating = 7); ‘People see themselves as stewards of the community’s well-being’ (baseline ‘Now’ rating = 4); ‘Stewards in our community are committed to change for the long term (baseline ‘Now’ rating = 3). They set their goals to increase each item by two points, to the next maturity level. In their action plan, strategies to address this included inviting new community-based organizations across the region to learning academies held by the coalition. These academies brought together community leaders to discuss salient regional health concerns, learn improvement methods, and create new collaborations. This coalition asked all health educators to co-Lead sessions at this event and encouraged rural health networks from surrounding counties to attend the event. One method for doing so was developing memorandums of understanding with expectations for rural representatives to be active in the event, incentivized by tying involvement to their community health improvement plans. To assess their success, they sent post-event surveys to attendees and received favorable feedback on the respondents’ comfort and confidence in working with their local health education.

As these activities took time to bear results, the coalition did not score themselves significantly higher during the second administration of the CTM. However, by the third and fourth administrations, they reported adding the largest county in their area to their collaboration, and perceived health educators as more involved and committed to local change. As a result, Coalition 3 rated the three CTM ‘shared stewardship’ items roughly the same at the first two administrations but felt confident enough to rate themselves higher by the third (8, 5, 5, respectively) and fourth (8, 6, 6, respectively) administration. At the same time, they also noted ongoing challenges of defining health educators’ roles in each county, engaging people with lived experience of inequities, and described that some counties were more advanced than others in collaboration and measurement, indicating further areas where work was needed. Used as intended, the CTM helped Coalition 3 to identify areas where they felt improvement was needed, to set goals toward these improvements, and to assess progress over time.”
CTM offers an adaptable, coalition-led process for understanding complex change. As such, it continues to be adapted and refined. For example, the Georgia Health Policy Center and County Health Rankings & Roadmaps adapted CTM items into the Assessment for Advancing Community Transformation, a self-assessment for communities to understand improvements in health and equity. With future applications, we can continue to learn how to make transformation manageable.
Hey You! Learn More
- The full CTM, along with information about SCALE, can be found here.
- To understand community transformation and the Community of Solutions framework, see here.
- See the recent publication “The Community Transformation Map: A Maturity Tool for Planning Change in Community Health Improvement for Equity and Well-Being” by Ariel Domlyn, Jonathan Scaccia, Niñon Lewis, Shemekka Ebony Coleman, Gareth Parry, Somava Saha, Abraham Wandersman, and Rohit Ramaswamy (2021). The full paper can be found in the American Journal of Orthopsychiatry, Volume 91 Number 3, pages 322-331, the full text of which can be found below
Leave a Reply